The most commonly reported adverse effects associated with Gabapentin are somnolence, dizziness, ataxia, fatigue, and dysphagia.
Nystagmus, tremor, diplopia, amblyopia, pharyngitis, rhinitis, dysarthria, nausea and vomiting, weight gain, edema, dyspepsia, amnesia, weakness, paraesthesia, arthralgia, myalgia, headache, purpura, leucopenia, anxiety, and urinary-tract infection may occur less frequently.
Rarely, pancreatitis, altered liver function tests, erythema multiforme, Stevens-Johnson syndrome, and blood glucose fluctuations in diabetics have been reported.
Common psychiatric effects include confusion, depression, and nervousness, and, more rarely, hallucinations and psychoses.
Other adverse effects include acute renal failure, allergic reactions, alopecia, angioedema, chest pain, hepatitis, jaundice, movement disorders such as choreoathetosis, dyskinesia and dystonia, palpitations, thrombocytopenia, and tinnitus.
An antiepileptic hypersensitivity syndrome, comprising fever, rash, eosinophilia, and lymphadenopathy, along with other organ involvement such as hepatitis, nephritis, hematological abnormalities, myocarditis, or myositis, has been associated with some antiepileptic drugs including Gabapentin.
Early manifestations, such as fever and/or lymphadenopathy, may be present without evident rash; patients with such signs or symptoms should be evaluated immediately and therapy stopped in the absence of a clear etiology.
Respiratory, thoracic and mediastinal disorders: Frequency "rare": Respiratory depression.


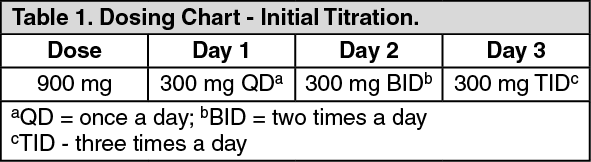 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image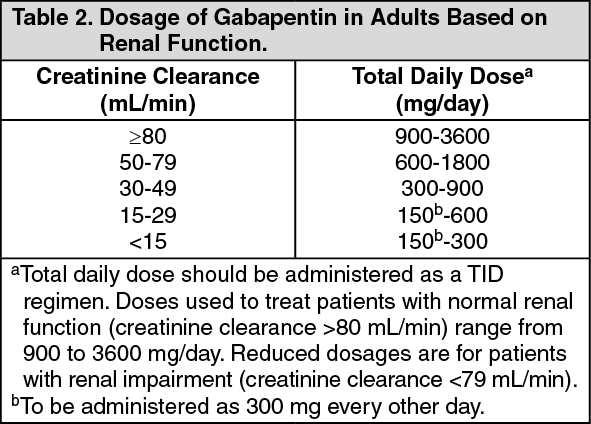 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
